I have only small items to add, as the knowledge (and almost certainly wisdom) of these writers exceeds mine. Read through before clicking any link, because you might decide to go in a different order. They are long and you might decide one or more is not worth your time, so wearr yourself out on the one you consider most important first.
This link from Random Critical Analysis, Why Conventional Wisdom on Health Care is Wrong (A Primer) was billed as the contrarian view on health spending as income increases in the third link of this post, which is where I originally started yesterday. I like it better than the last analysis, at least on that narrow section of the discussion. Maybe more than that, eventually. I am still thinking. Math is involved, including dealing with log-log scales, which give a different visual than what we are used to that might give you the wrong impression (even though they were a superior choice here). If you don't frequently use them (I used to. Very little now) I don't recommend you spend much time trying to get your head into the new space. Just be cautious about what you think your eyes are telling you about degree of differences. Similarly, if you aren't used to correlation coefficients, just pay attention to the relative numbers from -1.0 to 1.0, that 0.7 is a stronger correlation than 0.2, and the like. Getting close to 1.0 is a big deal, 0 is (heheh) nothing. It will do. In passing: it notes that when changes in income occur, the complex system takes 3-4 years to fully respond. This is something that is true of large mixed market systems in general. While some things respond rapidly, others take time. In America we ignore the latter because Elections, but that is a serious error on our part.
Let me add once more that medical care is more expensive because it can do more every year, and that does distribute broadly, even if somewhat unevenly, to the population. The lovely image of the town doctor pre-1940, making house calls and dispensing sage advice - and holding a ridiculously high status in the community compared to benefit given - misleads us. Doctors seem to have killed more patients than they saved until about 1940 when penicillin came in, which is even grimmer when we consider that germ theory and x-rays came in before those. So health care was cheap? It was also mostly useless. Whackadoodle theories, especially in Germany, sprang up at precisely the time that we were discovering that A) Science seems to work sometimes, and B) Doctors aren't doing any of that. So now we can do magic and it's expensive. You wouldn't pay a dollar now for what was top-of-the-line care in 1950.
From the later part of that article:
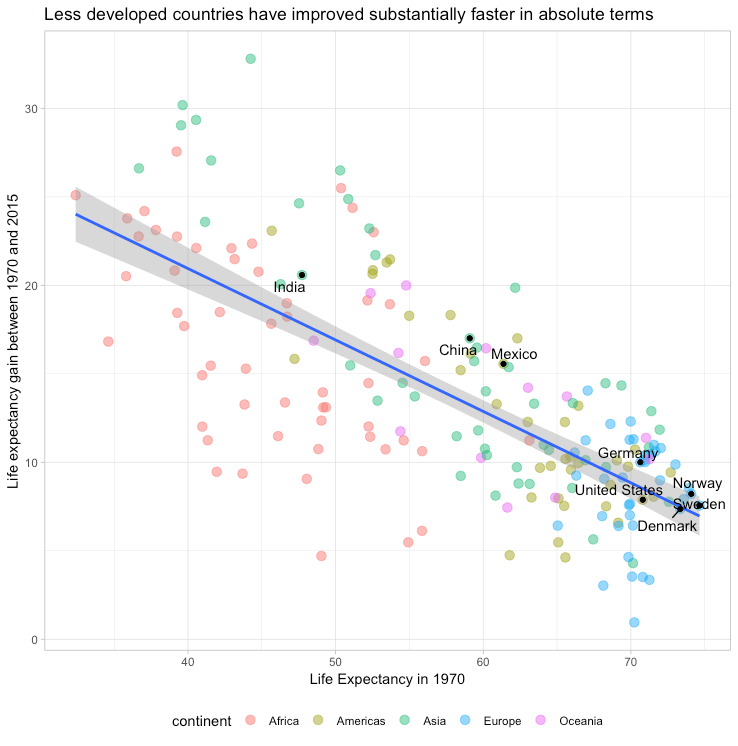
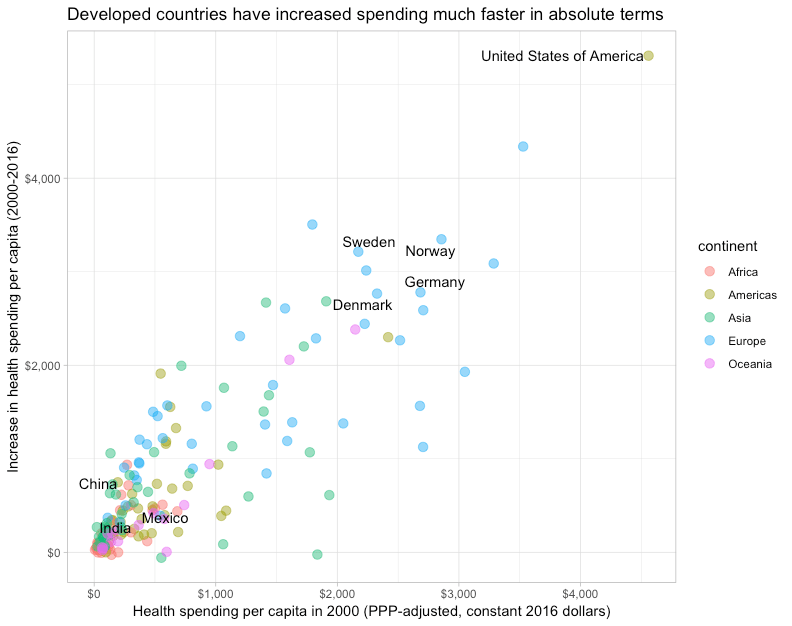
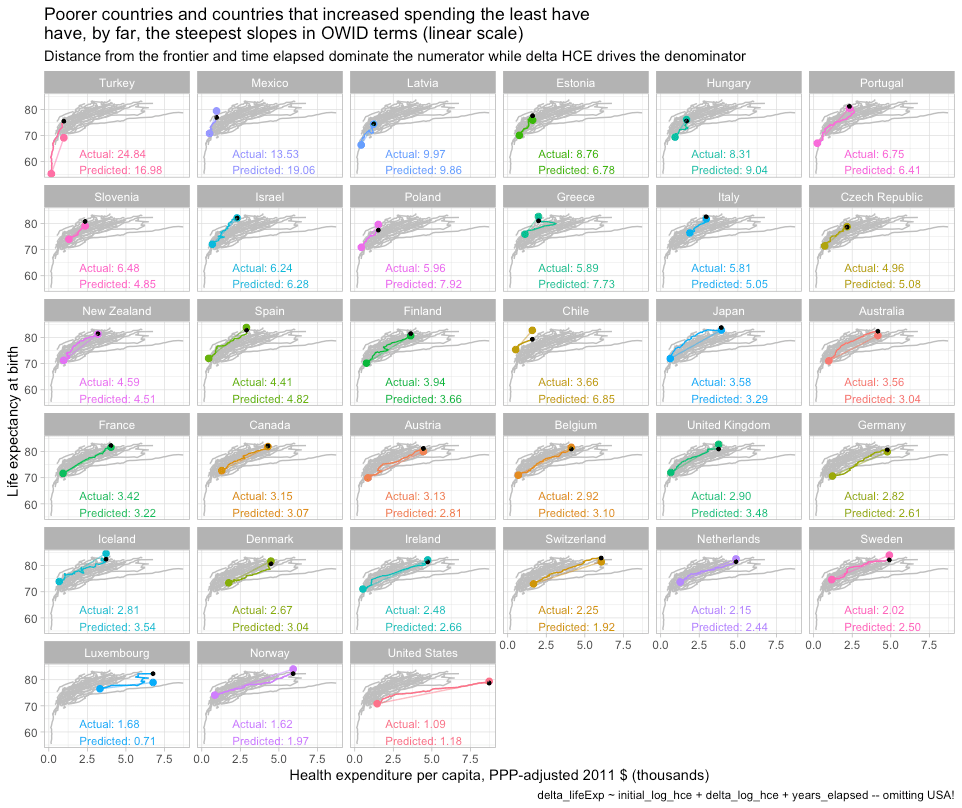
Likewise, the least developed parts of the world have converged rapidly on the most developed countries despite little-to-no convergence in income levels, health spending, and the like. Controlling for the change in health spending does not appreciably change these results. The supposedly radically divergent slope observed for the United States in widely circulated plots popularized by “Our World In Data” can be readily explained by distance from the frontier and the change in spending. America’s long-run rate of improvement in outcomes can be readily predicted based on patterns observed in other high-income countries — the US doesn’t even need to be included in the model to obtain such results.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Link to that whole final section, which is excellent.
Also it makes early reference to how GDP is not the best foundation for some of these analyses, though it is a very common one. It reminded me of this recent Quillette article The Mismeasure and Misuse of GDP. Even though it is more general, not specific to health care spending, there is some value.
The third link is where I started, from Astral Codex Ten Book Review: Which Country Has The World's Best Health Care? Excellent. My comments. The quick chart includes some things that have some neglected data beneath them. Life Expectancy at Birth may not be as clean a comparison as implied here. Western European and Anglospheric countries score very well. Some Northeast Asian countries (or regions) score just as well, others not. African countries have lower life expectancies, as do the Southeast Asian. The first two regions are richer, and this is usually considered the overwhelming reason for this. We don't like thinking there could be any racial substrate to this. Yet I think life expectancy is somewhat influenced by race. Infant mortality in the US is worse for those of African descent, but not worse for Hispanics, even when they are just as poor. In the world chart above, Latin American countries show better results than equally poor countries. Some wealthy Middle-Eastern countries still don't show out that well. I am not in any way suggesting that race is the primary driver. But looking at the numbers for China and Taiwan, which look very close to America' 78 years, it is worth remembering that Japan and South Korea have world-best expectancies, and America is the most racially mixed of the developed countries. So hold those numbers lightly.
Next, I can confirm that wait times for elective medicine are long in Norway, as one of my son's has had occasion to have to travel far with a two-night stay at a hotel to get elective surgery in eight months instead of 13 months. I hope they are otherwise as good as rated, as at the moment his girlfriend's son is in ICU there. Tom Bridgeland just reminded us of Canadians seeking care in America. Also, top US hospitals have Canadians seeking a second opinion coming down, even though they are paying out-of-pocket for this.
I also think that satisfaction is a slippery measure of a system. Americans complain about everything and find fault with it, even when it's basically fine. When things are deeply politicised, as they are in America as nowhere else on health care, this is even more pronounced. Whether you consider that valuable - always seeking improvement, or irritating - never happy with anything, is debatable. Scandis will always tell you how wonderful their countries are and how happy everyone is - but check the suicide rates.
Fun quote from that last essay by Scott Alexander
I would have appreciated a book by a more economically-minded person explaining why things are like this. Or maybe not; maybe it’s like quantum physics, and the second someone looks at it too closely, the whole structure will collapse, every hospital in the world will go bankrupt, and we’ll have to get our medical problems treated by wolves.
He wonders why countries who do things very similarly to the US have better results - contrary to what is politically asserted, that the US does things differently (usually, oh we're much worse, though the opposite occurs as well) from all other developed nations. In my ignorance, I do not wonder. We have many more people who game the system here. And that's not going away. Note also that AC10 has commenters from all over Europe and the Anglosphere who go into myths, advantages, and disadvantages of their own systems, which is valuable to those of us who are currently subjected to "Four legs good, two legs bad" in our debates here.
1 comment:
I'll have to go back and read the comments on Astral Codex Ten, I think I read it a bit too early for there to be many comments yet.
For reference material to have 'in my quiver' for the discussions I tend to have on healthcare, I think it is a great thing that this book & data are Zeke Emmanuel's -- his progressive credentials are unquestionable, and I find that the US people I tend to discuss policy with tend to disbelieve my facts, or assume them false if they come from a non-progressive source.
I've commented before elsewhere that in my discussion of national healthcare 'systems' with foreigners abroad, they don't believe me when I talk about Medicaid and EMTALA -- as their media has only ever told them that in the US if you are poor and without insurance, if you get sick or injured, you die. I know our safety net has gaps large enough to drive a supertanker through, and requires more patience with administravia than I'm usually willing to put up with personally, but I'm pretty sure I haven't imagined it full stop.
There is also a really strong sense in people I meet in their own countries that "the system in my country is best", even if the discussion originated in their relating some horrible preventable outcome that someone close to them experienced, and if the data demonstrate on many measurables that it performs poorly in comparison to other comparable places.
The UK NHS is a religious obsession -- my wife's father, brother, and sister-in-law are all doctors there, and she is imbued with the myth of 'tory cuts' to the NHS, and gets pretty angry with me when I show her data showing NHS funding has increased way more than inflation every year of my lifetime except during the time that Gordon Brown (Labour) was Prime Minister.
Having been hospitalized in Germany, I'm happy to see it at the top of the league table. That correlates with my anecdote.
Post a Comment